1- Introduction 2- Cellular level 3- Function 4- Pathphysiology 5- Clinical significance
(1)- Introduction --
-The stomach is a hollow organ that is part of the gastrointestinal system, and it is responsible for functions including the formation of chyme, synthesis of proteins necessary for vitamin absorption, microbial defenses, and propagates the peristaltic reflex. Contrary to popular thought, the stomach does not contribute to the absorption of any nutrients. This organ can is in the peritoneal cavity, located in the left upper abdominal quadrant or in the epigastric abdominal region that acts to relay ingested food between the nervous system and the endocrine system. Gastric acid secretion, peristaltic propulsion, and other physiologic functions of the stomach are finely controlled by the integration of the enteric nervous system, parasympathetic nervous system, and the secretion of various neurohormonal molecules (i.e., gastrin, HCl acid, intrinsic factor, bicarbonate, mucus, etc.)
- As a component of the alimentary canal (i.e., the tubal passageway for ingested food to be digested, absorbed, then excreted as waste), the stomach's physiological function is structured around creating an environment where the food ingested can be safely acted on by proteolytic enzymes and acidic solutions. There are pathologic consequences that can develop with the failure of the gastric mucosa to isolate the lumenal contents from the surrounding peritoneal cavity.
(2)- Cellular Level --
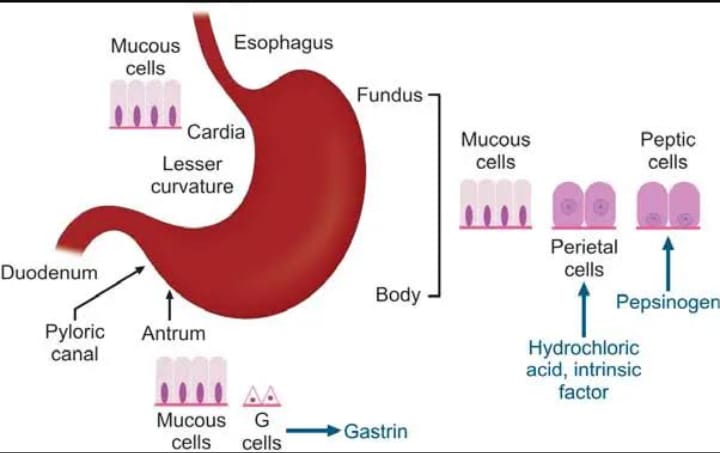
- As with most physiologic processes, the structure of an organ largely defines the function it contributes to the body. The gastric wall is specifically designed to aid in the formation of a transient acidic environment that allows for the digestion of food into a semisolid mixture called chyme. The stomach organ has four regions; fundus, cardia, body, and pylorus. The inner surface of the stomach is rugated to increase the surface area of the gastric mucosa allowing for gastric expansion with food ingestion. The wall of the stomach consists of four different tissue layers; mucosal layer, submucosa, muscularis externa, and adventitia/serosa. The gastric mucosal layer further subdivides into three layers; the surface epithelium, a connective tissue layer called the lamina propria, and the muscularis mucosa. The gastric epithelial layer invaginates into the lamina propria forming the gastric pits and glands. These gastric glands are lined with four specialized cells; surface mucous cells (foveolar cells), parietal cells, chief cells, and neuroendocrine cells (G-cells or ECL-like cells) that all contribute independent functions.
- The surface mucus cells (foveolar cells) are mucus-producing cells that primarily line the gastric mucosa. The secreted mucus acts as a barrier to the corrosive nature of the gastric acid. The rest of the specialized cells are found deep within the gastric glands (i.e., gastric pits).
. Parietal cells are specialized secretory epithelial cells that secrete gastric acid (HCl formation) into the lumen of the stomach through the gastric pits, primarily in the fundus. In addition to secreting HCl, the parietal cells secrete a protein called intrinsic factor. Intrinsic factor is necessary for the absorption of vitamin B12 in the terminal ileum of the small intestines. Three regulating molecules control these cells: acetylcholine (enteric nervous innervation) via muscarinic receptors, histamines (neuroendocrine cells) to histamine receptors, and gastrin (neuroendocrine cells) to gastrin receptors. All receptors appear on the basal side of the parietal cells, and they control a protein channel called H+/K+ ATPase on the lumenal side of the parietal cell. This protein transports one proton into the gastric lumen while intaking one K+ ion. Chloride ions follow the proton gradient via K+/Cl- channel into the gastric lumen leading to the formation of HCl.
. Chief cells are specialized secretory cells found at the base of the gastric glands within the fundus of the stomach that secrete the zymogen called pepsinogen. Pepsinogen is the inactive form of a proteolytic enzyme called pepsin, which is needed to digest proteins into small units called polypeptides. The zymogen pepsinogen only becomes activated by the gastric acid produced by the parietal cells. This mechanism acts as a safety measure to ensure the proteins found outside of the gastric lumen are not digested inappropriately. Chief cells are stimulated by cholinergic activity from the parasympathetic and by the hormone Gastrin.
.Neuroendocrine cells (i.e., enterochromaffin-like cells, or G-cells) are also found in the gastric glands on the gastric mucosa that secretes various molecules that aid in the production of gastric acid.
- The ECL-like cells produce and secrete Histamine when stimulated by a hormone called gastrin, which indirectly increases the HCl production byway of histamines' direct actions on the parietal cells. ECL-like cells are primarily located in the fundus of the stomach.
- G-cells are located in the pylorus region of the stomach, and they produce the neuroendocrine hormone called gastrin. Gastrin is capable of indirectly and directly increasing HCl production by two mechanisms. The first is by stimulation of the ECL-like cells to release Histamine, which then potentiates Parietal cells. The second is by direct stimulation of the Parietal cells themselves. Both mechanisms increase the H+/K+ ATPase activity.
- D-cells are located in the pylorus of the stomach, and they secrete an inhibitory molecule called Somatostatin. D cells are activated when the stomach lumen reaches a certain level of acidity. Somatostatin then acts to suppress the release of gastrin, reducing the overall production of gastric acid.
Compared to other organs of the GI tract, the stomach is unique in that its muscularis externa features an inner oblique layer in addition to a circular and longitudinal layer. Exterior to the submucosa is the submucosal Meissner's plexus, which controls secretions and blood flow. In between the circular and longitudinal layers of the muscularis externa is the myenteric Auerbach's plexus, which controls GI motility.
The right and left gastric arteries, left and right gastro-omental arteries, and short gastric arteries are responsible for blood supply to the stomach. Celiac ganglia and the vagus nerve innervate the stomach. The vagus nerve serves as an essential link between the brain and the gut respective to appetite control, acid secretion, and gastric motility.
(3)- Function --
- In addition to the stomach's secretory function, the stomach also has a muscular component, as do all structures within the alimentary canal. The muscularis externa is composed of smooth muscle cells that orient in three directions: oblique layer (unique to only the stomach), a circular muscle layer, and the longitudinal layer. Together these three muscle layers are responsible for the gastric movements needed to break the food bolus into smaller components. A food bolus, which consists of partially digested food from the mouth and the esophagus, is processed by the stomach into chyme, which is a more readily absorbable substance by the small intestine. The stomach accomplishes this food processing through forceful back-and-forth churning motions by the inner oblique layer of the muscularis externa. The circular and longitudinal layers facilitate gastric emptying of chyme through the pyloric sphincter, which allows only liquids and small enough food particles to pass through. Gastric emptying may be slowed by the presence of fats and acids in the duodenum, stress, exercise, and various hormones. Chyme that is not emptied will continue to churn in the stomach until it, too, can pass through the pyloric sphincter. Slow-wave contractions of the gastric smooth muscles are generated by myenteric interstitial cells of Cajal, which serve as GI pacemakers.
- There are three movements associated with gastric motility.
(1)- Peristaltic wave:
- Contraction of the longitudinal layer rhythmically - Peristalsis can only occur in a forward motion with receptive relaxation of the distal intestinal region.
(2)- Segmentation (i.e., mixing component):
- Rhythmic contraction of the circular muscle layer
- The myenteric plexus control sets the segmentation motor pattern as the pacemaker. Rhythmic transient depolarizations within this nervous system create a "waxing and waning" pattern of electrical amplitudes contributing to the formation of a "churning" motion. This motion is capable of slowing the speed of chyme progression through the system, thus allowing for optimal nutrient absorption.
(3)- Ancillary movements:
(1)- Stomach Relaxation: As a food bolus is transferred from the esophagus into the stomach lumen via the relaxation of the lower esophageal sphincter (LES), relaxation of the stomach is needed to allow for the accumulation of ingested food. The stomach acts as a temporary container so that the digestion of its contents can take place in a uniform and controlled manner. The relaxation occurs through the parasympathetic activation of the vagus nerve, which inhibits the contraction of the gastric muscle layer.
All mechanical movements are the result of coordinated muscle contractions. The muscle layer is regulated primarily by the enteric nervous system (ENS), which is the intrinsic nervous system of the alimentary canal. The ENS can become activated by various inputs from the CNS like olfaction, sight, mechanical reception of the food bolus, or chemical mediators (PSNS/SNS). The mesh-work of neurons that makes up the ENS is found between the longitudinal and circular muscle layers. Commonly, it is referred to as the Auerbach's plexus or the myenteric plexus. The degree and rate of peristalsis are established by the myenteric interstitial cells of Cajal (ICC), as previously mentioned.
- The stomach itself does not significantly contribute directly to the body's absorption of nutrients, although it absorbs some substances such as alcohol and aspirin. Parietal cells secrete intrinsic factor, which is essential in the absorption of vitamin B12 distally in the digestive tract by enterocytes of the terminal ileum.
Brief Cellular Review (refer to the "cellular" section for more information)
- Hydrochloric acid (HCl), the main constituent of gastric acid, is secreted by parietal cells. The hydrogen (H) and chloride (Cl) components of HCl are secreted separately by hydrogen/potassium ATPase pumps and chloride channels in the stomach. Pepsinogen, a proenzyme for pepsin, is secreted by chief cells. Collectively, gastric acid creates an acidic environment that denatures proteins and activates the conversion of pepsinogen to pepsin.[3] Pepsin breaks down proteins into smaller peptides, which may be further processed and later absorbed in the small intestine. The secretion of acid is under the regulation of both hormonal and neural components, including gastrin, histamine, prostaglandins, somatostatin, gastric inhibitory polypeptide, secretin, and the vagus nerve. Interventional inhibition of acid secretion to avoid various complications of excess acid is commonly done by administering proton pump inhibitors.
The acidic environment of the stomach is not only useful for protein denaturing but also for protection against potentially infectious agents. All material consumed by the body must pass through the stomach, making it an important defense against microbes. Many bacteria are killed or inhibited by the stomach's acidity.
Additionally, secretory cells of the gastric glands include foveolar cells and enteroendocrine cells. Foveolar cells protect the stomach from the corrosive nature of its acidic environment by producing mucus and bicarbonate (HCO3). Enteroendocrine cells secrete various digestive hormones such as gastrin, somatostatin, and ghrelin. Gastrin release occurs in response to increased gastric distension, increased gastric pH, and the presence of amino acids in the stomach.
Blood Supply and Lymphatics
(1)- Arterial Blood Supply:
- The celiac trunk, which is the first major branch of the aorta after the aorta traverses the diaphragm. The celiac trunk immediately divides into three predominant arteries: the common hepatic artery, the splenic artery, and the left gastric artery.
The left gastric artery runs the lesser curvature of the stomach and eventually anastomoses with the common hepatic artery. The greater curvature of the stomach receives vascular supply from the anastomoses of the left and right gastroepiploic arteries. The left originates as a branch of the splenic artery, and the right originates from the common hepatic artery.
(2)- Venous Drainage:
- The stomach predominately drains via the portal system to the liver before entering the inferior vena cava. The anastomoses drain the lesser curvature of the left and right gastric vein to the portal vein. The greater curvature is drained by the anastomoses between the left and right veins to the superior mesenteric vein, which eventually drains into the portal vein as well.
(3)- Lymphatic Drainage:
- The lymphatic vessels travel with the vasculature of the stomach along the lesser and greater curvatures of the stomach. Lymph fluid drains sequentially through several lymph node systems depending on the stomach region. Half of the fundus drains to the pancreaticolienal group, while the remaining half and the cardia drain to the Superior gastric group of lymph nodes. The body of the stomach drains to the inferior gastric subpyloric group of nodes, while the pyloric region drains to the suprapyloric group of nodes. All groups drain eventually into the celiac lymph node. Once the lymph is at the celiac node, the lymph drains through the cisterna chyli to the Thoracic duct where it returns to the heart.
(4)- Pathophysiology --
- The stomach is susceptible to several primary pathologies that all manifest with similar symptomatology of epigastric pain, burning, gnawing discomfort, nausea/vomiting (+/- blood), satiety, and distention. Pathologies can subdivide into the following categories:
(1)- Anatomical Pathologies:
(1)- Hypertrophic Pyloric Stenosis:
HPS is a condition that results from hyperplasia of the muscular layers in the mucosal wall of the pylorus in the stomach. The thickening of the pylorus leads to structural obstruction of the gastric outlet clinically presented with projectile nonbilious, non-bloody vomitus in an infant. Commonly, this condition develops in caucasian, first-born males around four weeks of age. Hypochloremic hypokalemic metabolic alkalosis develops from hydrochloric acid loss and the body's attempt to compensate for the alkalosis by increasing the renal tubular reabsorption of H+ ions, by eliminating K+ ions. On physical exam, a palpable epigastric mass, the shape, and size of an olive ("palpable olive") may be apparent. Definitive treatment is a surgical correction called a pyloromyotomy.
(2)- Ulcerative Pathologies:
(1)- Peptic Ulcer Disease:
- Gastric ulcers occur when the mucosa and submucosa of the stomach lining break down and are commonly due to H. pylori or long-term NSAID use. Less common causes include stress, diet, infection, and rarely, tumors. Often, ulcers are present in either the stomach mucosa (pain worsens after eating) or the duodenal mucosa (pain improves after eating). Patients often describe the pain as a burning or gnawing-type of pain felt in the epigastric region that may or may not radiate to the back. Patients who are clinically suspicious for peptic ulcer disease, an EGD (esophagogastroduodenoscopy) evaluation is a standard of care along with H. pylori testing. If H. pylori-positive, patient treatment will be with a proton pump inhibitor, amoxicillin, and clarithromycin. For penicillin-allergic patients, metronidazole can be an alternative. For H. pylori-negative patients with gastric ulcerations, further history should be obtained regarding NSAID use or other symptoms that could elucidate a potential etiology.
- The gold standard for testing is esophagogastroduodenoscopy (EGD). Management typically includes H2-receptor antagonists and proton pump inhibitors (PPIs).
(2)- Gastroesophageal Reflux Disease:
- Gastroesophageal reflux disease (GERD) is a common medical problem due to the reflux of gastric acid into the esophagus, causing symptoms or esophageal mucosal injury. Inappropriate relaxation of the lower esophageal sphincter is the common cause of reflux symptoms. The symptoms may include heartburn, regurgitation, dyspepsia, hoarseness, and chronic cough. Treatment will include weight loss and lifestyle changes to decrease the reflux or use of acid-reducing medications such as proton pump inhibitors.
(3)- Dyspepsia:
- Dyspepsia describes symptoms of indigestion, including nausea, vomiting, fullness, heartburn, belching, and abdominal pain. Functional dyspepsia refers to patients experiencing these symptoms in the absence of any clear cause. However, most cases of dyspepsia result from pathologies, a number of which involve the stomach.
(3)- Inflammatory Conditions:
(1)- Inflammatory Bowel Disease:
- Crohn disease is a non-caseating chronic granulomatous condition that is a type of inflammatory bowel disease. Crohn disease is capable of affecting any portion of the alimentary canal, from the mouth to the anus, including the stomach. Crohn disease is characterized by transmural inflammation that is non-continuous (skip lesions). Histologically, non-caseating granulomas are the hallmark finding. Endoscopy may show "cobblestoning" of the mucosa, mucosal strictures (i.e., string sign), or other sequelae throughout the GI tract. The terminal ileum is the most commonly affected region, but cases with gastric involvement have been noted with an incidence of <4>
(2)- Gastritis:
- Gastritis refers to gastric mucosa inflammation. Acute cases of gastritis are due to an imbalance between the stomach's acidic environment and its mucosal defense to the acid. This condition can arise with alcohol, chronic use of nonsteroidal anti-inflammatory drugs (NSAIDs), chemotherapy, decreased mucosal perfusion, or increased acid production. Chronic cases of gastritis involve atrophy of the gastric mucosa and intestinal metaplasia and primarily divide into two subtypes: autoimmune gastritis and bacterial gastritis. Autoimmune gastritis involves the autoimmune destruction of parietal cells, while bacterial gastritis refers to a gastric infection by Helicobacter pylori.
(3)- Helicobacter Gastritis:
- Helicobacter pylori (H. pylori) gram-negative bacteria is the primary pathogen responsible for peptic ulcers and gastric cancers (MALToma and adenocarcinoma) with a global prevalence of infection >50%. H. pylori-associated MALT lymphoma is incredibly unique in the fact that it is a type of cancer that can be treated effectively with antibiotics. H. pylori can colonize the stomach by neutralizing the acidic environment immediately surrounding the bacteria. The pathogen contains an enzyme called urease that is capable of converting urea to ammonia, which increases the pH, providing a protected environment until the pathogen can travel to and attach to the surface of the foveolar cells. Once anchored, the pathogen is protected by the mucus-buffer. Patients will present with epigastric burning, gnawing discomfort, dyspepsia, nighttime awakening, and relief with antacids. A urea breath test can determine if urease-positive bacteria have colonized the patient. Endoscopy is also recommended to evaluate for ulceration and intestinal metaplasia.
-Two widely accepted management regimens:
1... Triple Therapy: PPI + clarithromycin + amoxicillin (alt: metronidazole)
2... Quadruple Therapy: (history of previous macrolide exposure) PPI + bismuth subcitrate + metronidazole + tetracycline
(4)- Gastric Cancers:
- 90% of gastric cancers are determined to be adenocarcinomas with the remaining percentages divided between MALToma, carcinoid tumors, and stromal tumors.
- Gastric Adenocarcinoma
Two types of adenocarcinoma are common:
1... Intestinal Type: The intestinal type results from metaplasia and atrophy due to chronic gastritis, and is associated with smoking, alcohol, nitrosamines, and type A blood. Intestinal type tumors are typically intrusive growths on the lesser curvature of the stomach and may ulcerate.
2... Diffuse: The diffuse type is less common but characteristically results in a diffuse thickening of the gastric wall leading to a phenomenon called "linitis plastica."
- Gastric cancers are associated with several extra-systemic clinical findings, including acanthosis nigricans, Leser-Trelat sign, Virchow's node, Sister Mary Joseph's nodule, and Krukenberg tumors. Most gastric cancers are adenocarcinomas, and they most commonly metastasize to the liver.
- Management is mostly dependent on staging but commonly may involve tumor resection followed by adjuvant chemotherapy/radiation regimens. Gastric cancers have a good prognosis if the tumor is found early. However, most lesions are asymptomatic until later stages of disease progression.
(5)- Other Pathologies:
(1)- Menetrier's disease:
- Menetrier disease is hyperplasia of foveolar cells leading to overproduction of mucus, leading to excessive protein loss and minimal gastric acid production. Patient present with non-specific abdominal pain and edema. On endoscopy evaluation, gastric rugae will appear hypertrophied.
(2)- GAVE (Gastric Antral Vascular Ectasia):
- Angiodysplasia conditions leading to fragility of gastric blood vessels that are susceptible to rupture and bleeding. Patients can present with chronic anemia, GI bleeds, or hematemesis. On endoscopy, the lining of the stomach appears similar to the striations on a watermelon (i.e., watermelon stomach).
(3)- Gastroparesis:
- Gastroparesis is a condition where the gastric intrinsic nervous system called the enteric nervous system becomes impaired as a result of various etiologies like uncontrolled diabetes mellitus. Failure of the enteric nervous system fails the peristaltic contractions leading to stagnation of chyme propagation within and through the stomach. This condition can be idiopathic or caused by connective tissue disease, neurologic dysfunction, diabetes, infection, cancer, or obstruction.
(5)- Clinical Significance --
- Since everything the human body consumes by mouth passes through the stomach, it is exposed to a variety of foreign agents and is prone to homeostatic disruption. The prevalence of dyspepsia in the Western world is approximately 25%. Worldwide, gastric carcinoma is the fourth most common malignancy and the second deadliest. H. pylori, which causes multiple gastric disorders, remains a challenging infection to treat, and approximately 20% of H. pylori-infected people will continue to experience dyspepsia and may even develop extra-systemic diseases over their lifetime. Furthermore, with increasing rates of obesity worldwide, surgical manipulations of the stomach, such as bariatric surgery, are becoming more prevalent. Because of these factors, it is essential to continue increasing awareness and advancing the understanding of gastric function and disorders of the stomach.
Acid-reducing therapies had been the mainstay in the treatment of stomach related pathologies and symptoms varying from dyspepsia, GERD, gastritis to peptic ulcer diseases. Due to the high acidity or low pH (1.0) of gastric content, the simple antacids are commonly used and available over the counter. They are not effective except for transient relief of some symptoms. The antihistamine (H2 blockers) are more efficacious than acid-reducing therapies, and recently, there is greater, the widespread use of the most efficacious acid-reducing therapies, the proton pump inhibitors (PPI). PPIs are most effective in reducing acid production and help many symptoms related to gastric pathology. As a consequence, long-term use without clear indications is not uncommon. It is generally safe, yet the reduced acid-pepsin digestion of B12 containing food may lead to vitamin B12 deficiency, especially in the elderly and vegans.
2023 @ DL NEWS. All Rights Reserved.