In This Page.............
1- Introduction 2- Issuse of Concern 3- Cllular Level
4- Development 5- Organ Systems Involved 6- Function
7- Mechanism 8- Related Testing 9- Pathophysiology
10- Clinical Significance
(1)- Introduction --
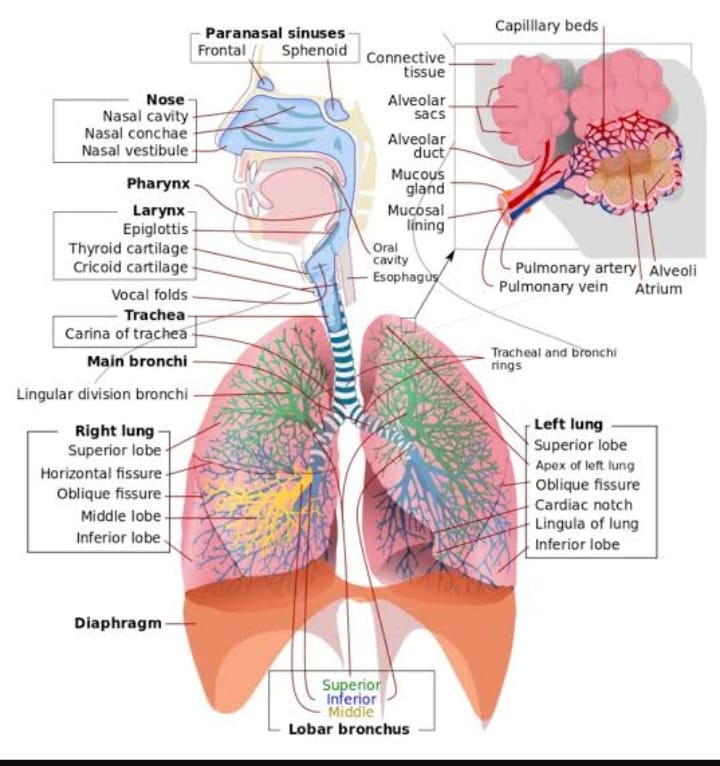
The lungs are the foundational organs of the respiratory system, whose most basic function is to facilitate gas exchange from the environment into the bloodstream. Oxygen gets transported through the alveoli into the capillary network, where it can enter the arterial system, ultimately to perfuse tissue. The respiratory system is composed primarily of the nose, oropharynx, larynx, trachea, bronchi, bronchioles and lungs. The lungs further divide into individual lobes, which ultimately subdivide into over 300 million alveoli. The alveoli are the primary location for gas exchange. The diaphragm is the primary respiratory muscle and receives innervation by the nerve roots of C3, C4, and C5 via the phrenic nerve. The external intercostals are inspiratory muscles used primarily during exercise and respiratory distress. The significant lung volumes/capacities and their definitions are listed below
1- Inspiratory reserve volume (IRV): Volume that can be breathed after a normal inspiration
2- Tidal volume (TV): Volume inspired and expired with each breath
3- Expiratory reserve volume (ERV): Volume that can be expired after a normal breath
4- Residual volume (RV): Volume remaining in lung after maximal expiration (cannot be measured by spirometry)
5- Inspiratory capacity (IC): Volume that can be breathed after normal exhalation
6- Functional residual capacity (FRC): Volume remaining in the lungs after normal expiration
7- Vital capacity (VC): Maximum volume able to be expired after maximal inspiration
8- Total lung capacity (TLC): Volume of air in the lungs after maximal inspiration
9- Forced expiratory volume (FEV1): Volume that can be expired in 1 second of maximum forced expiration
(1)- Issues of Concern --
The lung is a primary location for a large proportion of human disease. Lung disease further classifies into obstructive and restrictive disease.
(1)- Obstructive Disease:
The definition of obstructive disease is lung disease with impaired expiration. It presents with decreased FVC, decreased FEV1, and most notably, a dramatic decrease in FEV1/FVC. In obstructive disease, the air that should be expired is not, which leads to air trapping and an increased FRC. The two major examples of obstructive disease are listed below:
1- Asthma: a multifactorial disease characterized by chronic bronchial inflammation leading to eventual air trapping. Several key characteristics are as follows.
Airway disease is mostly reversible (i.e., with the administration of a beta-agonist).
Can cause chronic cough, wheeze, tachypnea, and dyspnea.
Chronic obstructive pulmonary disorder (COPD): a constellation of clinical symptoms that share features of both emphysema and chronic bronchitis leading to expiratory airflow limitation.
Chronic bronchitis demonstrates long-term airway inflammation causing excessive cough and sputum production.
Emphysema characteristically shows enlarged airspaces (loss of alveolar elasticity) leading to chronic dyspnea. The overly-distended airspaces prevent the lungs from adequately emptying.
Smoking is the primary cause of the disease and is directly related to the severity of the disease course.
Cigarettes induce inflammation in the lungs.
Airways show small airway disease and parenchymal destruction.
(2)- Restrictive Disease:
Restrictive lung disease is lung disease in which restricted lung expansion causes decreased lung volumes. Its characteristics include both a decreased FVC and decreased FEV1; however, the FEV1 is more reduced than FVC, causing FEV1/FVC to increase. Several examples of restrictive lung disease are listed below
1- Idiopathic pulmonary fibrosis
2- Pneumoconiosis
3- Sarcoidosis
(3)- Cellular Level --
Oxygen transport is the primary means by which the circulatory system perfuses tissue. Oxygen gets carried in the body in two major forms: bound to hemoglobin and dissolved. Hemoglobin is the major oxygen carrier in the body. The formula for the oxygen content of blood is as follows:
CaO2 = 1.34 x [Hgb] x (SaO2 / 100) + 0.003 x PaO2
CaO2 = oxygen content in blood
[Hb] = hemoglobin concentration
SaO2 = percentage of heme groups that are bound to oxygen
PaO2 = Partial pressure of oxygen
Four subunits comprise hemoglobin, each containing a heme-moiety that binds to iron. One molecule of O2 can bind to each iron atom of the heme group; therefore, each hemoglobin group can bind to four molecules of O2.
(4)- Development --
Lung development in-utero occurs in five main stages. The first stage begins with the development of the lung bud from the respiratory diverticulum during week 4 of embryogenesis. The stages are as follows.......
1- Embryonic: begins from weeks 4 to 7; this is when the formation of the major airways and pleura occur.
2- Psuedoglandular: occurs during weeks 5 to 17; this is when the bronchial tree and respiratory parenchyma form.
3- Canalicular: occurs during weeks 16 to 26; the distal airway, blood-air barrier, surfactant, and acini form.
4- Saccular: occurs during weeks 24 to 38 weeks; the airspaces (alveoli) continue to expand.
5- Alveolar: occurs from week 36 of gestation and throughout childhood. The alveoli become septated and more mature - improving airspace and capillary networks.
(5)- Organ Systems Involved --
The right ventricle conveys deoxygenated blood to the lungs via the pulmonary artery. The lungs will then breathe in air, which transfers oxygen through the alveoli into the dense capillary network surrounding the alveoli. The blood will then travel through the pulmonary vein into the left atrium, where it gets ejected from the left ventricle into the aorta. The aorta is the major artery that further branches into the system arteries, delivering blood to the cerebral, coronary, renal, splanchnic, and skin. Systemic veins return deoxygenated blood from these tissues to the vena cava, where it enters the right atrium and begins the cycle again.
The following equation can express blood flow dynamics: Q = P/R, where Q is the flow/cardiac output, P is the pressure gradient, and R is the total peripheral resistance.
(6)- Function --
The function of the pulmonary system is to extract oxygen from the environment and provide it for aerobic respiration at the cellular level. Oxygen is ultimately used to produce ATP, and carbon dioxide is breathed out with other metabolic byproducts.
Respiratory tract organs facilitate the process of gas exchange, including the nose, oral cavity, throat, trachea, bronchi, and lungs. The lungs divide into five major lobes: three lobes on the right and two lobes on the left. Each lobe is made up of many small alveoli, which are the primary site of gas exchange. At the alveoli, diffusion of gases into the arterioles occurs.
(7)- Mechanism --
The four significant aspects of respiratory mechanics are as follows: lung compliance, chest wall compliance, respiratory rate, and airway resistance. These work in conjunction to create a negative pressure within the lungs and pleural space, allowing air to be drawn into the lungs. Conversely, drops in lung volume increase pressure in the lungs, which forces air out.
The following equation represents lung compliance: C = V/P, where C is lung compliance, V is lung volume, and P is lung pressure.
Respiratory rate will adjust to meet the needs of the body. As oxygen demand increases and carbon dioxide builds up (i.e., exercise), the lungs will accommodate by increasing the respiratory rate to facilitate diffusion of these gases.
Chest wall compliance counteracts the force of lung compliance, attempting to increase lung volume (contrary to lung compliance where the lungs attempt to decrease volume)
Poiseuille’s law describes airway resistance, the law states: R = (8*n*l)/(pi * r ^4), where R = resistance, n = viscosity of air, l = length of the airway, and r = radius of the airway. It is essential to note the inverse fourth power relationship between the radius of the airway and the resistance. Small adjustments in airway radius will substantially alter the resistance.
(8)- Related Testing --
Pulmonary function tests (PFTs) serve a purpose both the investigation and monitoring of patients with pulmonary disease. They provide information relating to both large and small airways, lung parenchyma, and pulmonary capillary bed. PFTs are a safe and effective way to help the clinician diagnose and monitor pathology. There are many indications for PFTs, including:
1- Cough
2- Wheeze
3- Chest Xx-ray abnormalities
54- Shortness of breath
5- Crackles
6- Monitoring of patients with known respiratory disease (i.e., COPD, asthma, interstitial fibrosis)
7- Monitoring of diseases that may have associated respiratory complications (i.e., Guillain-Barre)
8- Perioperative evaluation
9- Lung transplant surveillance
10- The major measurements included in pulmonary function testing include FEV1, FVC, and FEV1/FVC. Some of the more common findings on PFTs are as follows.....
1- Interstitial fibrosis: dec. FVC, dec. FEV1, normal/ inc. FEV1/FVC
2- Asthma: dec. FVC, dec. FEV1, dec. FEV1/FVC
3- COPD: dec. FVC, dec. FEV1, dec. FEV1/FVC
(9)- Pathophysiology --
COPD is one of the major leading causes of lung pathology worldwide. Tobacco smoke is the primary cause of the disease. Nicotine and the thousands of other toxic components contained in cigarettes lead to the formation of free radicals, causing alveolar damage.
COPD is a general term referring to the combination of chronic bronchitis and emphysema. It is an obstructive disease, impairing expiration. The chronic bronchitis component causes severe hypoxemia due to airway inflammation and mucus production. The emphysematous component causes enlargement of air spaces, leading to decreased recoil and increased compliance, which ultimately causes air trapping.
(10)- Clinical Significance --
As lung pathology remains a significant cause of morbidity and mortality nationwide, understanding of basic lung physiology and its ties to pathology is essential for the clinician. Dysfunction of the pulmonary system ultimately leads to hypoxia. There are four classifications of hypoxia etiology:
1- Hypoventilation:
Any disease that decreases the ventilatory rate of alveoli ultimately results in hypoventilation. Several causes include obesity, CNS depressants, rib fractures, neurologic defects, and kyphoscoliosis.
2- Right-to-left-shunt:
The right-to-left shunt is when deoxygenated blood bypasses the lungs from the right heart to the left heart. This situation can occur both anatomically and physiologically. Anatomical causes of anatomical shunts include congenital heart malformations (i.e., tetralogy of Fallot) and arteriovenous malformations. Physiologic shunts occur when there is blood flow to an unventilated alveolus; this occurs in instances where air cannot diffuse across the alveolus, such as acute respiratory distress syndrome or pleural effusions.
3- V/Q mismatches:
V/Q mismatches occur when blood flow and ventilation are mismatched, as the name implies. Ideally, ventilation and perfusion match, for proper gas exchange. Normal V/Q ratio is 0.8. A high V/Q ratio occurs when ventilation exceeds perfusion. The classic example of this would be in a pulmonary embolism, where perfusion is completely blocked to a segment of lung, while ventilation remains unaffected. A low V/Q ratio occurs when there is normal blood flow to a region of the lung, but ventilation is blocked. An example of this would be in COPD, where the alveolus’ surface area is decreased, causing inadequate gas exchange.
4- Diffusion limitations:
Diffusion limitation occurs when oxygen cannot effectively move from the alveoli into the pulmonary capillaries. This condition can take place when there is the destruction of the alveoli (i.e., COPD), or in instances where there is destruction or thickening of the lung parenchyma (i.e., interstitial fibrosis). These commonly occur in conjunction with V/Q mismatches.
2023 @ DL NEWS. All Rights Reserved.