In This Page ...........
1- Introduction 2- Organ Systems Involved 3- Function
4- Related Testing 5- Pathophysiology 6- Clinical Significance
(1)- Introduction --
The cardiovascular system provides blood supply throughout the body. By responding to various stimuli, it can control the velocity and amount of blood carried through the vessels. The cardiovascular system consists of the heart, arteries, veins, and capillaries. The heart and vessels work together intricately to provide adequate blood flow to all parts of the body. The regulation of the cardiovascular system occurs via a myriad of stimuli, including changing blood volume, hormones, electrolytes, osmolarity, medications, adrenal glands, kidneys, and much more. The parasympathetic and sympathetic nervous systems also play a key role in the regulation of the cardiovascular system.
(2)- Organ Systems Involved --
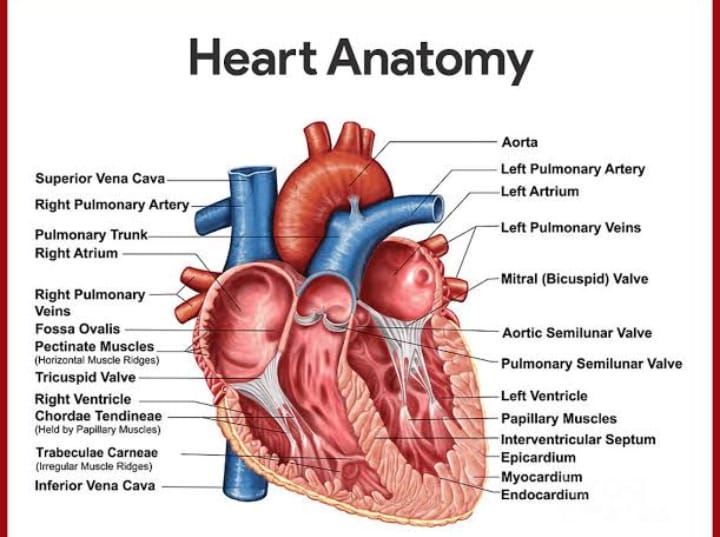
The heart is the organ that pumps blood through the vessels. It pumps blood directly into arteries, more specifically, the aorta or the pulmonary artery. Blood vessels are critical because they control the amount of blood flow to specific parts of the body. Blood vessels include arteries, capillaries, and veins. Arteries carry blood away from the heart and can divide into large and small arteries. Large arteries receive the highest pressure of blood flow and are thicker and more elastic to accommodate the high pressures. Smaller arteries, such as arterioles, have more smooth muscle, which contracts or relaxes to regulate blood flow to specific portions of the body. Arterioles face a smaller blood pressure, meaning they don't need to be as elastic. Arterioles account for most of the resistance in pulmonary circulation because they are more rigid than larger arteries. Furthermore, the capillaries branch off of arterioles and are a single-cell layer. This thin layer allows for the exchange of nutrients, gases, and waste with tissues and organs. Also, the veins transport blood back to the heart. They contain valves to prevent the backflow of blood.
(3)- Function --
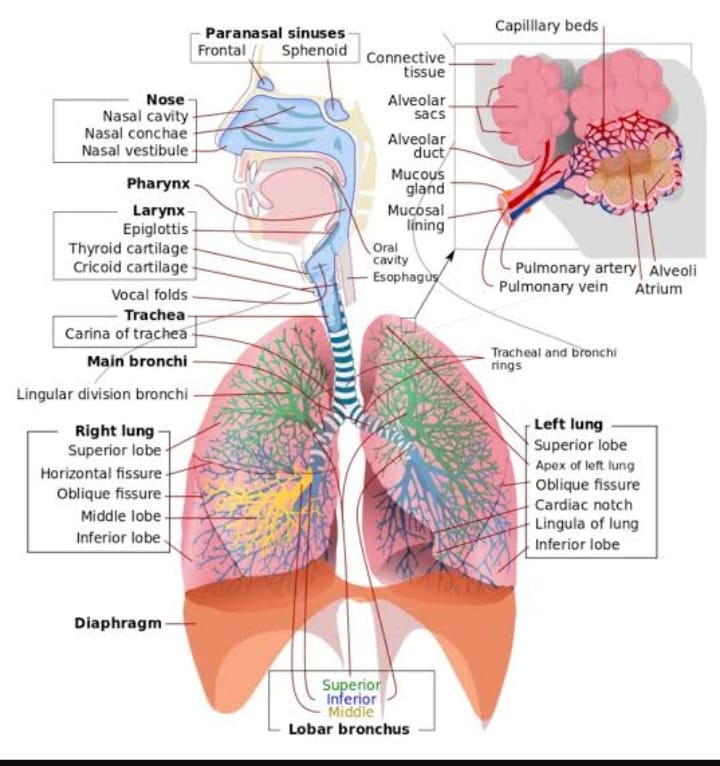
The cardiovascular system consists of two main loops, systemic circulation, and pulmonary circulation. The purpose of the cardiovascular system is to provide adequate circulation of blood through the body. Pulmonary circulation allows for the oxygenation of the blood, and systemic circulation provides for oxygenated blood and nutrients to reach the rest of the body.
(4)- Mechanism --
It is important to understand the concept of cardiac output, stroke volume, preload, Frank-Starling law, afterload, and ejection fraction to understand the physiology of the heart. The cardiac output (CO) is the amount of blood ejected from the left ventricle, and normally it is equal to the venous return. The calculation is CO = stroke volume (SV) x heart rate (HR). CO also equals the rate of oxygen consumption divided by the difference in arterial and venous oxygen content. The stroke volume is the amount of blood pumped out of the heart after one contraction. It is the difference in end-diastolic (EDV) and end-systolic volume (ESV). It increases with increased contractility, increased preload, and decreased afterload. Also, contractility of the left ventricle increases with catecholamines by increasing intracellular calcium ions and lowering extracellular sodium. The preload is the pressure on the ventricular muscle by the ventricular EDV. Frank-Starling law describes the relationship between EDV and SV. This law states that the heart attempts to equalize CO with venous return. As venous return increases, there is a larger EDV in the left ventricle, which leads to further stretching of the ventricle. Further stretching of the ventricle leads to a larger contraction force and a larger SV. A larger stroke volume leads to a larger CO, thus equalizing CO with venous return. Next, the afterload is the pressure that the left ventricular pressure must exceed to push blood forward. Mean arterial pressure best estimates this. Also, afterload can be estimated by the minimum amount of pressure needed to open the aortic valve, which is equivalent to the diastolic pressure. Thus, diastolic blood pressure is one of the better ways to index afterload. Finally, the ejection fraction (EF) is equal to SV/EDV. EF of the left ventricle is an index for contractility. A normal EF is greater than 55%. A low EF indicates heart failure.
The cardiac cycle describes the path of the blood through the heart. It runs in the following order:
Atrial contraction closure of the mitral valve
Isovolumetric phase
Opening of the aortic valve
Ejection phase (rapid and reduced ejection), emptying of the left ventricle
Closure of the aortic valve
Isovolumetric relaxation
The opening of the mitral valve
Filling phase (rapid and reduced filling) of the left ventricle
Vasculature plays a significant role in the regulation of blood flow throughout the body. In general, blood pressure decreases from arteries to veins, and this is because of the pressure overcoming the resistance of the vessels. The greater the change in resistance at any point in the vasculature, the greater the loss of pressure at that point. Arterioles have the most increase in resistance and cause the largest decrease in blood pressure. The constriction of arterioles increases resistance, which causes a decrease in blood flow to downstream capillaries and a larger decrease in blood pressure. Dilation of arterioles causes a decrease in resistance, increasing blood flow to downstream capillaries and a smaller decrease in blood pressure. Diastolic blood pressure (DP) is the lowest pressure in an artery at the beginning of the cardiac cycle while the ventricles are relaxing and filling. DP is directly proportional to total peripheral resistance (TPR). Also, the energy stored in the compliant aorta during systole is now released by the recoil of the aortic wall during diastole, thus increasing diastolic pressure. Systolic blood pressure (SP) is the peak pressure in an artery at the end of the cardiac cycle while the ventricles are contracting. Directly related to stroke volume, as stroke volume increases, SP also increases. SP is also affected by aortic compliance. Because the aorta is elastic, it stretches and stores the energy caused by ventricular contraction and decreases the systolic pressure. Pulse pressure is the difference between SP and DP. Pulse pressure is proportional to SV and inversely proportional to arterial compliance. Thus the stiffer the artery, the larger the pulse pressure. Mean arterial pressure (MAP) is the average pressure in the arteries throughout the cardiac cycle. The MAP is always closer to DP. MAP is calculated by MAP= DP + 1/3 (pulse pressure). Also, MAP = CO x TPR, where CO is cardiac output. This value is significant because whenever there is a decrease in CO, to maintain the MAP, the TPR will increase, which is relevant in many pathophysiology problems.
Systemic veins have a lower decrease in pressure because it has low resistance. The venous system is very compliant and contains up to 70% of the circulating blood at once. A small change in venous pressure can mobilize the blood stored in the venous system. Velocity of blood in the vasculature has an inverse relationship with cross-sectional area (volumetric flow rate (Q) = flow velocity (v) x cross-sectional area (A)). As the cross-sectional area increases, velocity decreases. Arteries and veins have smaller cross-sectional areas and the highest velocities, whereas capillaries have the most cross-sectional area and the lowest velocities. The vasculature also gives resistance. Resistance is R= (8*viscosity*length)/(πr^4). Viscosity depends on hematocrit and increases in multiple myeloma or polycythemia. As tube length increases, the resistance increases. As the tube radius increases, the resistance decreases. The fact that the radius is to the power of 4 means that slight changes in the radius have a profound effect on resistance. The total resistance of vessels in a series is R1 + R2 + R3, and so on, and the total resistance of arteries in parallel is 1/TR = 1/R1+1/R2+1/R and so on, where TR is the total resistance.
The Poiseuille equation measures the flow of blood through a vessel. It is measured by the change in pressure divided by resistance: Flow = (P1 - P2)/R, where P is pressure, and R is resistance. Increasing resistance in a vessel, such as the constriction of an arteriole, causes a decrease in blood flow across the arteriole. At the same time, there is a larger decrease in pressure across this point because the pressure is lost by overcoming the resistance. Increasing the resistance at any point increases upstream pressure but decreases downstream pressure. The Poiseuille equation applies to the systemic circulation such that F is the cardiac output (CO), P1 is the mean arterial pressure (MAP), P2 is the right atrial pressure (RAP), and R is the total peripheral resistance (TPR). Because RAP is close to 0 and very small in comparison to MAP, the equation approximates as F=P1/R or CO=MAP/TPR where MAP=CO*TPR - this means that cardiac output and total peripheral resistance control MAP. Its application is important because in trauma situations with hemorrhage, there is also a decrease in cardiac output, but at times the blood pressure is near normal. This is because the TPR at the level of the arterioles has increased. This equation, as applied to the pulmonary vasculature, is used to determine the cause of pulmonary hypertension. As related to the pulmonary vasculature, F represents CO, P1 represents pulmonary artery pressure (PAP), and P2 represents left atrial pressure (LAP), and R is pulmonary vascular resistance (PR); CO=(PAP-LAP)/PR. A Swan-Ganz catheter helps to measure both PAP and LAP, allowing for the measurement of PR and, thus, the etiology of pulmonary hypertension.
The nervous system regulates the cardiovascular system with the help of baroreceptors and chemoreceptors. Both receptors are located in the carotids and aortic arch. Also, both have afferent signals through the vagus nerve from the aortic arch and afferent signals through the glossopharyngeal nerve from the carotids.
Baroreceptors are more specifically located in the carotid sinus and aortic arch. They respond quickly to changes in blood pressure.
A decrease in blood pressure or blood volume causes hypotension, which leads to a decrease in arterial pressure, which creates a decrease in the stretch of the baroreceptors and decreases afferent baroreceptor signaling. This decrease in afferent signaling from the baroreceptor causes an increase in efferent sympathetic activity and a reduction in parasympathetic activity, which leads to vasoconstriction, increased heart rate, increased contractility, and an increase in BP. The vasoconstriction increases TPR in the equation MAP=CO*TPR to bring pressure (MAP) back up.
An increase in blood pressure or blood volume causes hypertension which increases the stretch of the baroreceptors
Chemoreceptors come in 2 types: peripheral and central. Peripheral chemoreceptors are specifically located in the carotid body and aortic arch. They respond to oxygen levels, carbon dioxide levels, and the pH of the blood. They become stimulated when oxygen decreases, carbon dioxide increases, and the pH decreases. Central chemoreceptors are located in the medulla oblongata and measure the pH and carbon dioxide changes in the cerebral spinal fluid.
Autoregulation
Autoregulation is the method by which an organ or tissue maintains blood flow despite a change in perfusion pressure. When blood flow becomes decreased to an organ, arterioles dilate to reduce resistance.
Myogenic theory: Myogenic regulation is intrinsic to the vascular smooth muscle. When there is an increase in perfusion, the vascular smooth muscle is stretched. This causes it to constrict the artery. If there is a decrease in perfusion to the arteriole, then there is decreased stretching of the smooth muscle. This leads to the relaxation of the smooth muscles and dilation of the arteriole.
Metabolic theory: Blood flow is closely related to metabolic activity. When there is an increase in metabolism to muscle or any tissue, there is an increase in blood flow to that location. Metabolic activity creates substances that are vasoactive and stimulate vasodilation. The increase or decrease in metabolism leads to an increase or decrease in metabolic byproducts that cause vasodilation. Increased adenosine, carbon dioxide, potassium, hydrogen ion, lactic acid levels, and decreased oxygen levels, and increased oxygen demand all lead to vasodilation. Adenosine is from AMP, which derives from the hydrolysis of ATP and increases during hypoxia or increased oxygen consumption. Potassium is increased extracellularly during metabolic activity (muscle contraction) and has a direct effect on relaxing smooth muscles. Carbon dioxide is produced as a byproduct of the oxidative pathway and increases with metabolic activity. Carbon dioxide diffuses to vascular smooth muscle and triggers an intracellular pathway to relax the vascular smooth muscle.
Heart: Metabolites that cause coronary vasodilation include adenosine, NO, carbon dioxide, and low oxygen.
Brain: The primary metabolite controlling cerebral blood flow is carbon dioxide. An increase in arterial carbon dioxide causes vasodilation of cerebral vasculature. A decrease in arterial carbon dioxide causes vasoconstriction of the cerebral vasculature. Hydrogen ions do not cross the blood-brain barrier and thus are not a factor in regulating cerebral blood flow. A decrease in oxygen pressure in arteries causes vasodilation of the cerebral arteries; however, an increase in oxygen pressure in arteries does not cause vasoconstriction.
Kidneys: Autoregulation of the kidneys is myogenic and with tubuloglomerular feedback. In severe cases of hypotension, kidney arterioles constrict, and renal function is lost.
Lungs: Hypoxia of the lungs causes vasoconstriction, creating a shunt away from poorly ventilated areas of the lung and redirecting perfusion to ventilated portions of the lung.
Skeletal muscle: Adenosine, potassium, hydrogen ion, lactate, and carbon dioxide all increase during exercise and cause vasodilation. When resting, the skeletal muscle is controlled extrinsically by sympathetic activity and not by metabolites.
Skin: Regulation of the skin occurs through sympathetic stimulation. The purpose of regulating blood flow in the skin is to regulate body temperature. In a warm environment, skin vasculature dilates due to a decrease in sympathetic stimulation. In cold environments, skin vasculature constricts due to an increase in sympathetic activity. During fever, regulation of the body temperature is at a higher setpoint.
The starling equation can explain the capillary fluid exchange. This equation describes the forces of oncotic and hydrostatic pressure on the movement of fluid across the capillary membrane. Edema can result from an increase in capillary pressure (heart failure), a decrease in plasma proteins (liver failure), an increase in the interstitial fluid due to lymphatic blockage, or an increase in capillary permeability due to infections or burns.
(5)- Related Testing --
Swan-Ganz catheter is a thin tube that is inserted peripherally and passed to the right side of the heart and into the pulmonary artery. This catheterization is to measure the pressures in the pulmonary vasculature and the left atrium. Pulmonary capillary wedge pressure (PCWP) is an estimate of the pressure in the left atrium given by the Swanz-Ganz catheter. It is significant because it helps to differentiate pathologies. In cardiac shock, there is an increase in PCWP, whereas in hemorrhagic shock, there is a decrease in PCWP.
(6)- Pathophysiology --
Chronic hypertension is a common pathological process related to the cardiovascular system. This condition is significant because, with hypertension, there is an increase in afterload. A long-term increase in afterload leads to concentric hypertrophy of the heart and eventual left-sided diastolic heart failure. Also, an S4 heart sound will be audible at the apex of the heart. Another type of heart disease is alcoholic cardiomyopathy, which occurs in alcoholics and causes dilated cardiomyopathy, which means the ventricles become dilated, leading to systolic failure. It can be reversible if the patient stops drinking alcohol.
Heart failure or cardiac tamponade can cause cardiogenic shock. In cardiogenic shock, there is an increase in PCWP because there is a backup of blood; the heart is not able to pump blood forward because it is not able to overcome the afterload. Subsequently, there is a decrease in CO. In response to low CO, the SVR increases.
In hemorrhagic shock, there is a loss of blood, thus a loss in total volume. Because there is a loss of volume, there is a decrease in pressure and, therefore, a decrease in PCWP. Also, there is an increase in cardiac output because there is a need for more blood in the periphery. While there is an increase in CO, there is also an increase in SVR to maintain MAP.
(7)- Clinical Significance --
Blood pressure (BP) is an essential clinical value because it describes the status of the vasculature in acute and chronic states. If a patient has elevated blood pressure in the clinic on more than two occasions, the clinician can diagnose the patient with essential hypertension. BP can also be significant in acute settings, such as in the emergency room, after a patient is brought in by an ambulance due to a motor vehicle accident. At this point, it is important to assess the patient's BP because if it is low, it might indicate the patient is bleeding somewhere, and the clinician must determine the location of the bleeding as soon as possible.
S1 and S2 heart sounds are normal heart sounds heard on auscultation of the heart. S1 is the sound made due to the closure of the mitral and tricuspid valves. This is followed by systole. Then the S2 sounds are heard, which are the closure of the aortic and pulmonary valves. Diastole follows this. It is important to recognize these normal heart sounds on auscultation because abnormal heart sounds such as S3, S4, and murmurs can be signs of a pathological condition
2023 @ DL NEWS. All Rights Reserved.