1- Introduction --
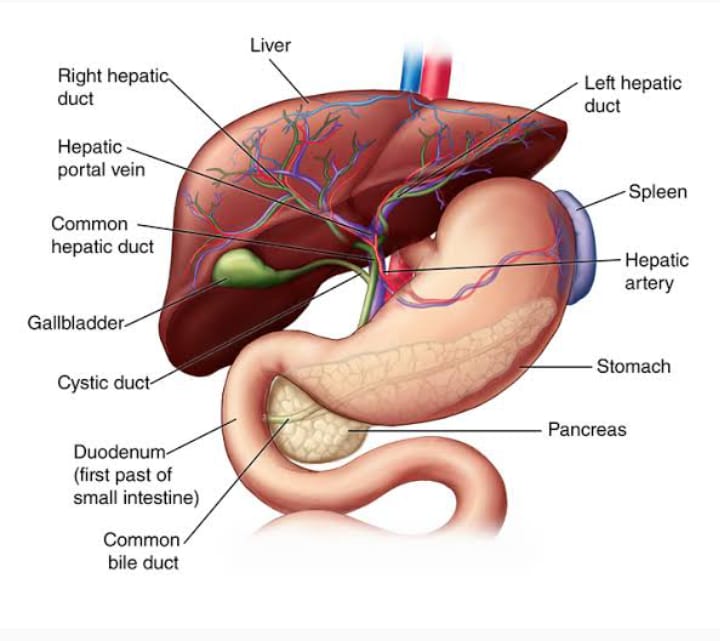
The liver is a critical organ in the human body that is responsible for an array of functions that help support metabolism, immunity, digestion, detoxification, vitamin storage among other functions. It comprises around 2% of an adult's body weight. The liver is a unique organ due to its dual blood supply from the portal vein (approximately 75%) and the hepatic artery (approximately 25%).
2- Cellular Level --
The functional unit of the liver is the lobule. Each lobule is hexagonal and a portal triad (portal vein, hepatic artery, bile duct) sits at each corner of the hexagon. The foundation of the lobule is composed of hepatocytes, which have physiologically distinct apical and basolateral membranes. Based on function and perfusion, hepatocytes are divided into 3 zones
(1). Zone I is considered to be the periportal region of hepatocytes and are the best perfused and first to regenerate due to their proximity to oxygenated blood and nutrients. Due to its high perfusion, zone I plays a large role in oxidative metabolisms such as beta-oxidation, gluconeogenesis, bile cholesterol formation, and amino acid catabolism.
(2). Zone II is defined as the pericentral region of the hepatocytes and zone II sits between zones I and III.
(3). Zone III has the lowest perfusion due to its distance from the portal triad. It plays the largest role in detoxification, biotransformation of drugs, ketogenesis, glycolysis, lipogenesis, glycogen synthesis, and glutamine formation.
Bile flow is further facilitated by bile canaliculi, which are formed by apical membranes of neighboring hepatocytes. Due to the 3-dimensional arrangements of hepatocytes, the canaliculi form a lattice-like network or “chicken-wire pattern,” that helps increase the surface area of flow. It is important to recognize that bile and blood flow in opposite directions to each other. This makes sense as the liver produces bile, so bile in the ducts are leaving the liver; whereas, the dual blood supply is entering the liver to perfuse it. Blood drains into the branch of the hepatic vein that lies in the lobule's center via sinusoidal lumens of the lobule.
The space between the sinusoidal lumen and the surrounding basolateral membrane of hepatocytes is called the space of Disse. This space is occupied by microvilli extending from the basolateral membrane of the hepatocytes that communicate with the capillary, allowing the hepatocyte to reach its' blood supply. The space of Disse houses an extracellular matrix composed of a variety of collagens, proteoglycans, and other proteins that help provide scaffolding for the hepatocytes and, by extension, the lobule as a whole. The importance of the scaffolding that takes place in the space of Disse is amplified further by the fact that hepatocytes do not contain a true basement membrane. The space of Disse also contains Kupffer cells (macrophages) and Ito cells (stellate cells). The Kupffer cells sit in the space to filter out unnecessary or pathologic material from the circulation. The Ito cells serve as storage for fat, such as vitamin A. In the right setting, they can also serve as myofibroblasts and aid in the regeneration of the liver.
3- Development --
The liver arises as a part of the foregut. It stems from endodermal cells and starts as the hepatic diverticulum around the fourth week of development. It forms within the peritoneum and is anchored to the abdominal wall by the falciform ligament which arises from the ventral mesentery. The umbilical vein passes through the falciform ligament on its way from the umbilical cord to the liver.
The diverticulum is believed to be induced by a combination of several pathways, mainly the Wnt/B-catenin pathway and fibroblast growth factors (FGF), which are secreted by fetal cardiac cells, which is induced by the MAPK pathway. The diverticulum then grows and interacts with the septum transversum, a structure that divides the heart from the abdominal cavity and later contributes to the formation of the diaphragm. The diverticulum then differentiates into the primordium of the liver or the gallbladder. As the primordium liver grows, it develops into hepatic cords that anastomose around spaces lined by endothelium, forming the primordium of the hepatic sinusoids. VEGF plays an important role in the formation of the hepatic sinusoids.
The portal vein, which arises from umbilical and vitelline veins is the central vessel in which the hepatic cords form around. This helps explain why the portal vein is the primary blood supply for the liver as opposed to the hepatic artery. The hepatic artery develops with the biliary tract and continues to develop post-birth. Around the sixth week, the liver becomes responsible for hematopoiesis, and hepatocytes create bile around the 12th week.
4- Organ Systems Involved --
The liver plays a role in nearly every organ system in the body. It interacts with the endocrine and gastrointestinal systems by aiding in digestion and metabolism. The liver is the storage location for fat-soluble vitamins and handles cholesterol homeostasis. It stores iron and copper. It plays a role in hematology with clotting factor and protein synthesis. The liver plays a role in heme breakdown into unconjugated bilirubin and conjugates it. It plays a role in sex hormone metabolism and produces carrier proteins that are important in reproduction and development. Finally, Kupffer cells and Pit cells play an important role in the body’s immunologic system.
5- Function --
(1)- Bile Production -- Bile is an important fluid as it helps excrete material not excreted by the kidneys and aids in the absorption and digestion of lipids via secretion of bile salts and acids. Bile is produced by hepatocytes and is mainly composed of water, electrolytes, bile salts, bile acids, cholesterol, bile pigment, bilirubin, and phospholipids in addition to other substances. Bile is secreted from hepatocytes into the bile canaliculi where it travels from smaller ducts to the larger ducts eventually ending up in the duodenum or being stored in the gallbladder for storage and concentration as determined by the duct and sphincter of Oddi pressures. Following secretion of bile into the duodenum, it undergoes enterohepatic circulation, where it performs its job in the bowel, and bile components that are not excreted are recycled by conversion into bile acids by gut bacteria for reuse by absorption in the ileum and transport back to the liver.
(2)- Fat-Soluble Vitamin Storage and/or Metabolism -- Most fat-soluble vitamins reach the liver via intestinal absorption in the form of chylomicrons or VLDL. The liver stores and/or metabolizes fat-soluble vitamins. As discussed earlier, vitamin A is stored in Ito cells. It can undergo oxidation into retinal followed by retinoic acid for phototransduction, or retinoic acid can be conjugated into glucuronide for secretion into bile. Whether vitamin D3 comes from the skin, animal products, or plant products, it must undergo 25-hydroxylation by the hepatic CYP-450 system, which is further hydroxylated in the kidney to achieve its functional form. The hepatic CYP-450 system then hydroxylates carbon 24 to render vitamin D inactive. The liver receives vitamin E in its alpha and gamma-tocopherol forms. Alpha-tocopherol is integrated with VLDL or HDL in the liver and is then secreted back into circulation while the liver metabolizes the gamma-tocopherol form for excretion. While vitamin K is not stored or metabolized in the liver, its presence is essential as the liver enzyme, gamma-glutamyl carboxylase requires it for gamma-carboxylation of coagulation factors II, VII, IX, X, and protein C and protein S.
(3)- Drug Metabolism -- Another critical function of the liver is metabolism and/or detoxification of xenobiotics. The liver uses lysosomes for some of these substances, but a major route of metabolism and detoxification is through biotransformation. The liver functions to transform xenobiotics mainly by converting them from a lipophilic form to a hydrophilic form through 2 reactions: phase I and phase II. These reactions mainly take place in the smooth endoplasmic reticulum of hepatocytes. Phase I reactions create a more hydrophilic solute via oxidation, reduction, and hydrolysis using primarily the cytochrome P450 (CYP450) family of enzymes. The product of phase I has an oxygen species that reacts better with enzymes involved with phase II reactions. Phase II reactions conjugate the metabolites created in phase I to make them more hydrophilic for secretion into blood or bile. There are three main avenues for conjugation performed in phase II reactions: conjugation to glucuronate, glutathione, or sulfate. Conjugation to glucuronate, such as with bilirubin, takes place in the smooth endoplasmic reticulum. Substances undergoing sulfate conjugation, such as alcohols, are usually done in the cytosol due to the location of the needed enzymes. Most glutathione conjugation occurs in the cytosol, with a minority occurring in the mitochondria. It is essential that glutathione is reduced and depletion of reduced glutathione for conjugation can allow the buildup of toxic metabolites as seen in acetaminophen overdose. Some describe the transport of metabolites produced from these reactions as phase III. Other organs, such as the kidney and gut can aid in drug metabolism. Multiple factors such as age, gender, drug-drug interactions, diabetes, pregnancy, liver or kidney disease, inflammation, or genetics to name a few, affect drug metabolism.
(4)- Bilirubin Metabolism -- The liver plays a significant role in the breakdown of heme. Hemolysis takes place in multiple locations throughout the body, including the liver, spleen, and bone marrow. Heme is broken down into biliverdin, which is then reduced to unconjugated bilirubin. The liver receives unconjugated bilirubin bound to albumin from the circulation. The unconjugated bilirubin then undergoes conjugation via the uridine diphosphate glucuronyltransferase (UGT) system, a phase II process, to become hydrophilic. The newly conjugated bilirubin then is secreted via bile canaliculi into the bile or small amounts dissolve in the blood where it then gets filtered for excretion by the kidneys. Most conjugated bilirubin enters the bile and is excreted with bile in feces as it is not absorbable by the intestinal wall. Some bilirubin is converted to urobilinogen or unconjugated bilirubin by gut bacteria for reabsorption to undergo enterohepatic circulation.
(5)- Other Functions -- The liver plays a role in thyroid hormone function as the site of deiodination of T4 to T3. The liver manages the synthesis of nearly every plasma protein in the body, some examples include albumin, binding globulins, protein C, protein S, and all the clotting factors of the intrinsic and extrinsic pathways besides factor VIII.
6- Related Testing --
Liver function tests (LFTs) are a commonly ordered panel among clinicians to help assess a patient’s liver. While its components, aspartate transaminase (AST), alanine transaminase (ALT), bilirubin, alkaline phosphatase, and gamma-glutamyltranspeptidase (GGT) help portray a portrait of what is occurring in the liver, the panel merely identifies the degree of cell damage if any, occurring in the liver. The reason these levels better reflect the presence of injury is that these enzymes are components of hepatocytes that get released into the circulation upon hepatocyte damage. ALT and AST are important enzymes in gluconeogenesis, with ALT being more specific for the liver as AST is found in a variety of tissues. Alkaline phosphatase (ALP) can be found in the bone as well as the biliary tree, so it is not as specific, but when used in combination with the rest of the panel, it supplies evidence of hepatocellular injury. In particular, elevated ALP signals damage to the lining of the biliary tract.
A true test to assess the liver’s function is its ability to synthesize protein. While albumin is an important protein the liver produces, albumin levels do not only provide an idea of how the liver is functioning, but its levels are also influenced by other factors, such as nutrition status and nephrotic syndromes. In addition, albumin has a half-life of 15 to 20 days and therefore may not identify acute liver dysfunction. As such, albumin levels are combined with coagulation studies to provide insight into the liver’s functional capacity. All clotting factors except for factor VIII are produced by the liver. The coagulation proteins used in the extrinsic pathway are tested with the PT test. These factors must be carboxylated in the liver, with a pathway that uses vitamin K, meaning an elevated PT could signal liver damage, vitamin K deficiency or current warfarin therapy.
Ultrasound is an inexpensive and noninvasive imaging modality commonly used in the assessment of the liver. Most commonly, right upper quadrant ultrasounds are used to assess the biliary tree for obstruction and/or inflammation, such as in cholecystitis or choledocholithiasis. Ultrasound has the ability to reveal various liver pathologies and show various characteristics, such as border regularity, solid or cystic, and location.
Triple phase imaging such as computed tomography (CT) or magnetic resonance imaging (MRI) studies is used to characterize and diagnose liver lesions. These studies use contrast and scan images at specific time points to gather a portal venous phase, arterial phase, and venous phase. Depending on how the lesion takes up the contrast, clinicians can better diagnose the lesion, sometimes without needing to perform invasive procedures, such as needle biopsy. For example, hepatocellular carcinoma (HCC) as discussed below, demonstrates arterial hyperenhancement in most cases as they gather their blood supply from the hepatic artery. While CT is generally cheaper, MRI may be more beneficial due to its ability to show soft tissue better, potentially detailing the lesion better.
7- Pathophysiology --
Cirrhosis is a result of continuous liver injury, inflammation, fibrosis, and necrosis. Alcoholism and chronic hepatitis B and C commonly cause cirrhosis. Hepatitis C is the most damaging. The fibrosis present in cirrhosis occurs from the secretion of TGF-beta from the Ito cells in the space of Disse.
Cirrhosis usually represents with end-stage liver disease and, as such, liver function is greatly compromised. The diminished ability to produce protein and detoxify substances results in symptoms of portal hypertension, hyperestrinism, and hypoalbuminemia. Decreased clotting factor synthesis results in coagulopathy. Its presentation arises from manifestations from diminished hepatic function and portal hypertension.
Sequelae of portal hypertension include portosystemic shunts that result in varices in various locations, caput medusae, and hemorrhoids. Other manifestations of portal hypertension include ascites, spider angiomas, hepatic encephalopathy, hepatorenal syndrome, and splenomegaly. Esophageal varices are the most common cause of death in cirrhotic patients.
The Child-Pugh score and model for end-stage liver disease (MELD) score are both used to assess and determine prognosis in cirrhotic patients. Both look at a combination of variables to score the patient. The Child-Pugh score evaluates ascites, hepatic encephalopathy (HE), total bilirubin, albumin, and prothrombin time or INR. The MELD score uses creatinine, bilirubin, and INR. While both are used to create a predictive model for cirrhotic patients, the MELD score is the scale of choice for the evaluation of liver transplant patients.
Jaundice is often a sign of altered bilirubin metabolism. The first sign of jaundice is often yellowing under the tongue, followed by scleral icterus (yellowing of the sclera). There are numerous causes for jaundice, which can typically be classified by getting a fractionated bilirubin where indirect bilirubin (unconjugated bilirubin) and direct bilirubin (conjugated bilirubin) are measured. The result of the fractionated bilirubin can help identify the etiology of the cholestasis into prehepatic and intrahepatic or extrahepatic causes.
A common etiology of prehepatic jaundice is hemolysis where the level of hemolysis overwhelms the conjugating capacity of the liver, resulting in a buildup of unconjugated bilirubin, causing jaundice. Causes of intrahepatic cholestasis can be congenital diseases, such as Gilbert syndrome, and Crigler-Najjar syndrome. In these congenital diseases, the enzyme responsible for bilirubin conjugation, UGT, is mildly deficient or completely deficient, respectively. Dubin-Johnson and Rotor syndrome are causes of direct bilirubinemia as there is a defect in canalicular transport of conjugated bilirubin. Other causes of post-hepatic cholestasis are an obstruction, such as due to a stone or malignancy. Viral hepatitis can result in both indirect and direct hyperbilirubinemia.
8- Clinical Significance --
A variety of viruses can lead to liver damage. Hepatitis viruses A and E lead to acute hepatitis without resulting in chronic hepatitis, although hepatitis E can lead to fulminant hepatitis in pregnant patients. Hepatitis A and E are typically seen in travelers and from contaminated water or seafood sources. They are usually self-limiting illnesses that present with jaundice and vomiting. Hepatitis B, C, and D are viruses that can cause acute hepatitis that result in chronic hepatitis. Hepatitis D relies on hepatitis B for reproduction. It can either occur at the same time as hepatitis B, called coinfection, or on top of hepatitis B, called superinfection. The distinction is important as superinfection can lead to more severe disease. Hepatitis B and C can both occur from contaminated needles, as in tattoos, intravenous drug use, or iatrogenically. Hepatitis B can also be sexually transmitted. The best treatment for hepatitis A, B, and C is vaccination, and IgG is a marker that shows vaccination or prior exposure, whereas IgM shows acute infection. There have been advancements in the treatment of hepatitis C, to where it can be cured using combination antiviral agents like sofosbuvir/velpatasavir.
Primary biliary cholangitis (PBC) formerly known as primary biliary cirrhosis, is believed to be an autoimmune disease leading to chronic liver disease, eventually leading to end-stage liver disease and cirrhosis. It is most commonly seen in middle-aged women. Like other liver diseases, PBC can present with right upper quadrant and/or discomfort. Laboratory workup can reveal nonspecific elevations in liver enzymes. Anti-mitochondrial antibodies are the most specific marker for PBC and can be detected via ELISA. Treatment for PBC includes ursodeoxycholic acid to slow disease progression and other medications targeted at immune modulation such as methotrexate, steroids, and in some situations, calcineurin 2 inhibitors. A liver transplant is the only curative treatment.
Alcoholism has deleterious long-term effects on the liver. The liver is responsible for the breakdown of alcohol and over time, constant alcohol use leads to cell injury due to toxic metabolite buildup, usually from acetaldehyde. As this process continues, the liver becomes cirrhotic, developing all the features of cirrhosis discussed above. Diagnosis is clinical and can be accomplished via clinical history, physical exam findings, laboratory findings, as well as questionnaires. Screening in clinics can be performed using the CAGE questionnaire. A paper and pencil questionnaire that can be administered is the AUDIT. Alcoholism can present with symptoms of portal hypertension as mentioned above, alcohol withdrawal, delirium tremens, or complications, such as Wernicke encephalopathy, Korsakoff syndrome, and hepatic encephalopathy. Some laboratory biomarkers used to assess for alcoholism include AST, ALT with the classic ratio of AST/ALT being 2:1, GGT, MCV, blood alcohol, and ethyl glucuronide. Treatment is centered around behavioral modification, usually with alcoholics anonymous, and can be supplemented by medications, such as disulfiram.
Besides malignant lesions, there are a variety of benign liver lesions. The four most commonly discussed are hemangiomas, which are the most common, focal nodular hyperplasia (FNH), hepatocellular adenomas, and hepatic cysts. FNH occurs in the setting of congenital vascular formations or vascular disruptions and it is not uncommon for them to be seen in association with hemangiomas. These can be differentiated from hemangiomas macroscopically based on the presence of a central stellate scar and do not have as high of a risk of rupture that hemangiomas do. Imaging workup specific for FNH if prior workup is ambiguous includes sulfur colloid imaging or use of eovist. Hepatocellular adenomas are well-defined lesions that are frequently caused by oral contraceptives and anabolic steroids and can grow during pregnancy. Treatment is centered on discontinuing known causative agents. They are only very rarely premalignant in the healthy population. There is an association of glycogen storage disorders with hepatocellular adenomas, which are more dangerous as there is an increased frequency of transformation into hepatocellular carcinoma in these situations. Overall management can be conservative with serial imaging, but adenoma must be resected if greater than 5 cm, male gender, or the lesion is bleeding. If the patient is not an ideal surgical candidate, embolization can be performed.
liver is susceptible to malignancy. Most cases of malignancy involving the liver are a result of metastasis to the liver due to it receiving blood from so much of the body. The most common primary malignancy of the liver is hepatocellular carcinoma. As discussed, HCC can arise from hepatocellular adenomas, but can also arise from cirrhosis, which occurs for a variety of reasons, such as primary biliary cirrhosis, alcoholism, NAFLD, chronic hepatitis B or C and more. Treatment for any malignant lesion depends on the patient’s clinical picture and involvement of the liver; if not too much of the liver is involved, resection and embolization or microwave ablation can be performed. Otherwise, systemic chemotherapy/radiation can be performed to minimize tumor burden.
Non-alcoholic, fatty liver disease (NAFLD) is a spectrum of liver disease ranging from benign steatosis to cirrhosis requiring a liver transplant. It is one of the most common chronic liver conditions necessitating a liver transplant. There are a variety of causes of NAFLD, ranging from metabolic syndrome, pregnancy, nutrition, drugs, toxins, and more. It is most commonly seen in diabetics and obese patients. It can also present in asymptomatic patients receiving workup for other reasons. It can sometimes present with right upper quadrant pain and/or discomfort. Liver enzymes can be elevated, classically with an elevated ALT:AST ratio. It is managed with lifestyle modification of diet, exercise, and weight loss. This can be further augmented by pharmacologic treatment with drugs that target insulin resistance like metformin, thiazolidinediones, lipid modulators, and vitamin E, which serves as an anti-oxidant.
2023 @ DL NEWS. All Rights Reserved.